Vistogard® (uridine triacetate) oral granules can be taken mixed in foods, such as
applesauce, pudding, or yogurt
Chewing the VISTOGARD granules is not recommended
If the patient vomits within 2 hours of taking a dose of VISTOGARD, the patient should
take another complete dose as soon as possible after vomiting and the next dose at the
regularly scheduled time
If the patient misses a dose at the scheduled time, take that dose of VISTOGARD as
soon as possible. Then take the next dose at the regularly scheduled time
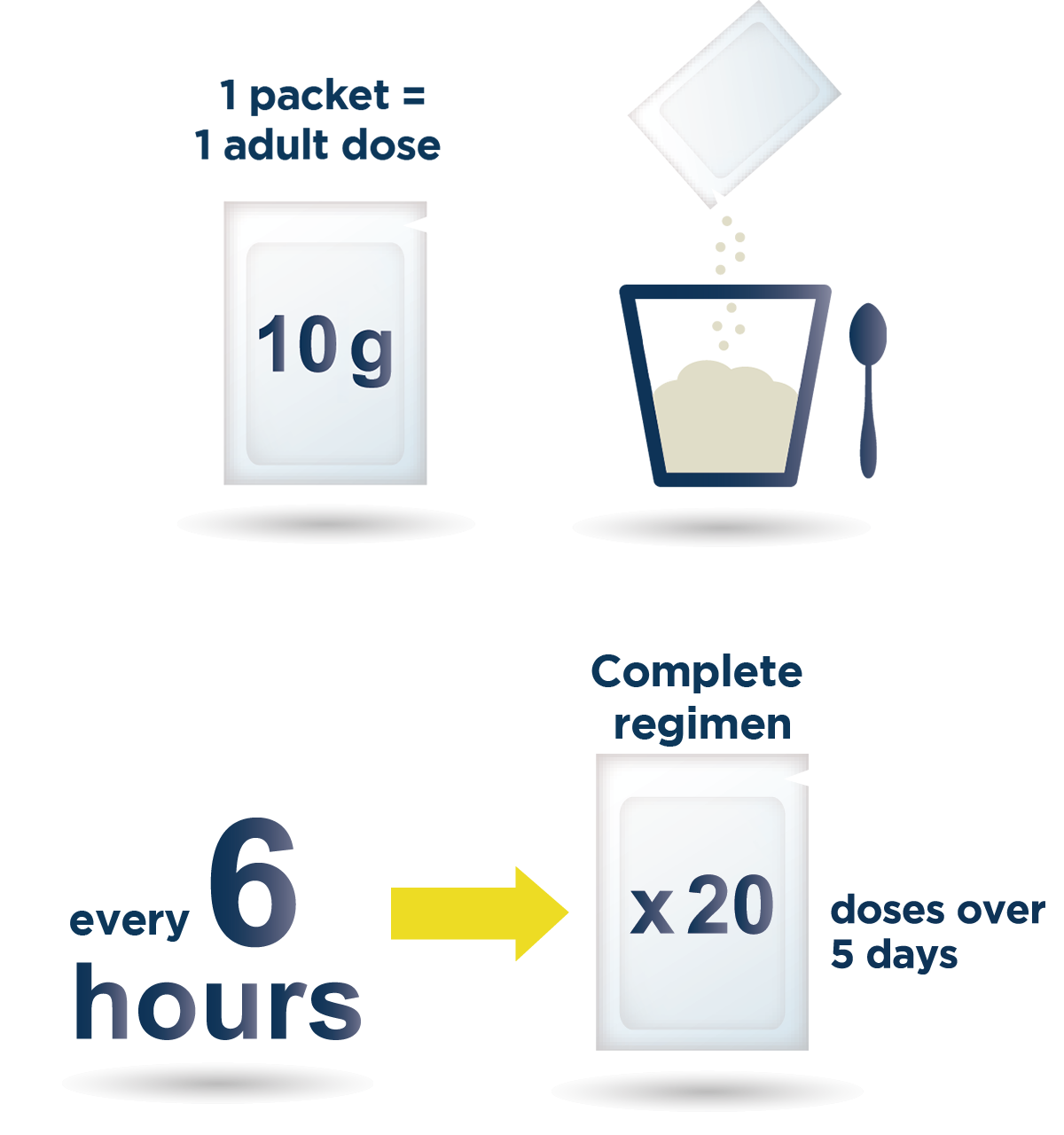
Administer all 20 doses of VISTOGARD, even if the patient
feels well1
If treatment is delayed until symptoms appear, they may be irreversible3
Median duration of exposure was 4.8 days, with a median of 20 doses (range, 1-23) in
clinical trials including both inpatients and outpatients1,11
Special dosing instructions1
VISTOGARD may be administered via nasogastric tube (NG tube) or gastrostomy tube
(G-tube) when necessary (eg, severe mucositis or coma)
The pediatric dose is 6.2 g/m2 of body surface area (not to
exceed 10 g/dose) orally every 6 hours for 20 doses, without regard to meals
Measure the dose using either a scale accurate to ≥0.1 g or a graduated teaspoon
accurate to ¼ teaspoon
Discard any unused portion of granules. Do not use granules left in the open packet
for subsequent dosing
Pediatric dose based on body surface area1
Patient body surface area (m2)
VISTOGARD 6.2 g/m2/dose*
Dose in grams
Dose in graduated teaspoons
0.34 to 0.44
2.1 to 2.7
1
0.45 to 0.55
2.8 to 3.4
1 ¼
0.56 to 0.66
3.5 to 4.1
1 ½
0.67 to 0.77
4.2 to 4.8
1 ¾
0.78 to 0.88
4.9 to 5.4
2
0.89 to 0.99
5.5 to 6.1
2 ¼
1.00 to 1.10
6.2 to 6.8
2 ½
1.11 to 1.21
6.9 to 7.5
2 ¾
1.22 to 1.32
7.6 to 8.1
3
1.33 to 1.43
8.2 to 8.8
3 ¼
1.44 and above†
10.0
1 full packet†
*Dose by body surface area category in this table was rounded to achieve
the approximate dose. Each dose is administered every 6 hours for 20 doses.1
†May use 1 entire 10 g packet without weighing or measuring. Do not
exceed 10 g/dose.1
SERB® and the SERB logo are registered trademarks of SERB S.à.r.l.
Vistogard® is a registered trademark of BTG International Inc., a SERB Pharmaceuticals company.
If you wish to report an adverse event or product quality complaint, please call 1-877-377-3784.
You are encouraged to report side effects of prescription drugs to the FDA.
Ma WW, Saif MW, El-Rayes, BF et al (2017), Emergency Use of
Uridine Triacetate for the Prevention and Treatment of Life-Threatening
5-Fluorouracil and Capecitabine Toxicity. Cancer 123(2):345-356
Ison G et al. (2016), FDA approval: Uridine triacetate for the treatment
ofpatients following fluorouracil or capecitabine overdose or exhibiting
early-onset severe toxicides following administration of these drugs. Clin
Cancer Res 22(18): 1-5
Brutcher E et al. (2018) Assessment and Treatment of Uncommon, Early-
onset, Severe Toxicides Associated With 5-Fluorouracil and
Capecitabine. Clin J Oncology Nursing 22 (6): 627-634
Polk A. et al. (2016). Incidence and risk factors for capecitabine-induced
symptomatic cardiotoxicity: A retrospective study o f452 consecutive
patients with metastatic breast cancer. BMJ Open, 6, e012798
Genentech, Inc. (2016). Xeloda® (capecitabine) Package Insert
Meulendijks, D et al. (2016) Renal function, body surface area, and age
are associated with risk of early-onset fluoropyrimidine-associated
oxicity in patients treated with capecitabine-based anticancer regimens
in daily clinical care. European Journal of Cancer, 54, 120-130
Froehlich TK et al. (2015). Clinical importance of risk variants in the
dihydropyrimidine dehydrogenase gene for the prediction of early-onset
fluoropyrimidine toxicity. International Journal of Cancer, 136, 730-739
Mitani S et al. (2017) Acute hyperammonemic encephalopathy after
fluoropyrimidine-based chemotherapy: A case series and review of the
literature Medicine 96:22(e6874)
Etienne-Grimaldi M-C et al. (2017) New advances in DPYD genotype
and risk of severe toxicity under capecitabine. PLOS ONE, 12, e0175998
Hamzic S et al. (2018) Come a long way, still a ways to go: from
predicting and preventing fluoropyrimidine toxicity to increased
efficacy? Pharmacogenomics 19(8):689-692 Published Online: 22 May
2018
Rodriguez RU. Public teleconference regarding licensing and
collaborative research opportunities for: methods and compositions
relating to detecting dihydropyrimidine dehydrogenase (DPD). Fed
Regist. 2008; 73(129):38233
Andre T et al. (2004) Oxaliplatin, fluorouracil, and leucovorin as
adjuvant treatment for colon cancer N Engl J Med. 2004;350: 2343-2351
Sara JD et al. (2018) 5-fluorouracil and cardiotoxicity: a review
Therapeutic Advances in Medical Oncology Vol 10: 1-18
Peng J et al. (2018) Cardiotoxicity of 5-fluorouracil and capecitabine in
Chinese patients: a prospective study Cancer Communications; 38(22):
1-7
Yeh KH and Cheng AL (1997) High-dose 5-fluorouracil infusional
herapy is associated with hyperammonaemia, lactic acidosis and
encephalopathy Brit. J Cancer 75(3): 464-465
Cordier P-Y et al. (2011). 5-FU-induced neurotoxicity in cancer patients
with profound DPD deficiency syndrome: A report of two cases. Cancer
Chemotherapy and Pharmacology, 68, 823-826
BTG International Inc. (2023) Vistogard (uridine triacetate) Oral Granules Package Insert
Garcia R et al. (2018) Prompt treatment with uridine triacetate improves
survival and reduces toxicity due to fluorouracil and capecitabine
overdose or dihydropyrimidine dehydrogenase deficiency Toxicology
and Applied Pharmacology 353 (2018) 67-73
Baldeo C et al. (2018) Uridine triacetate for severe 5-fluorouracil
toxicity in a patient with thymidylate synthase gene variation: Potential
pharmacogenomic implications (Case Report). SAGE Open Medical
Case Reports Volume 6: 1-4
Vaudo CE et al. (2016) Early-Onset 5-Fluorouracil Toxicity in a Patient
Negative for Dihydropyrimidine Dehydrogenase Mutations: The Clinical
Course of Reversal with Uridine Triacetate. Pharmacotherapy 36(11)
e178-e182
Santos C et al. (2017) The successful treatment of 5-fluorouracil (5-FU)
overdose in a patient with malignancy and HIV/AIDS with uridine
triacetate. American Journal of Emergency Medicine 35(5) 802.e7-
802.e8
Chu E (2014) Epidemiology and natural history of central venous access
device use and infusion pump function in the NO16966 trial Brit J Cancer
110, 1438-1445 doi: 10.1038/bjc
You are now leaving the patient site.
The section you selected contains information intended for U.S. healthcare professionals only.
Please certify that you are a U.S. healthcare professional by clicking the link below.